Blueprint for Breakthroughs is a LinkedIn newsletter published by Adrienne B. Mendoza, MHA, SVP BioBridge Global and Chief Operating Officer (COO), BBG Advanced Therapies
Originally published on LinkedIn on June 17, 2025, Adrienne discusses the importance of scaling the process of advanced therapies while keeping GMP quality
Patient-specific manufacturing is one of the most exciting and most complex challenges in cell and gene therapy. Each batch is made for one person. Each run requires exact timing, coordination, and quality control. But as more of these therapies move closer to commercialization, the challenge isn’t just how to manufacture them…it’s how to make them scalable, affordable, and accessible at the same time.
We’re not the first industry to face this problem. From custom dental aligners to personalized lenses and even automated drug packaging, other sectors have figured out how to deliver mass customization without compromise by building smart, closed, and repeatable systems that still allow for individualized outcomes and GMP quality.
In this edition of Blueprint for Breakthroughs, I teamed up with several of my colleagues to explore what the shift toward closed, decentralized systems could mean for advanced therapies—and what lessons we can borrow from the industries that have already made that leap. Their insights bring real-world context to the challenges and opportunities ahead: Henry Sentmore shares his perspective on the pressure cleanrooms place on single-patient production; Robert Reese offers insight into designing processes with closure in mind from the start; John Ibarra reflects on the precision and coordination required for patient-specific manufacturing runs; and Rogelio Zamilpa provides a broader view on cost, scalability, and the operational models that can support a more accessible future.
Why Cleanrooms Still Matter – But Shouldn’t Limit Us
In most cases today, cleanrooms are still the cornerstone of GMP production for advanced therapies. They’re tightly regulated, controlled environments that enable:
- Aseptic handling
- Manual interventions
- Process customization during early-stage trials
But they also introduce challenges:
- High cost per square foot
- Long lead times for availability
- Labor-intensive operations
- Scheduling constraints, especially in individualized production models
“Following strict protocols in the cleanroom is vital to our client’s success in manufacturing life saving therapeutics. Operating efficiently while sticking to strict c GMP on top of layered garments is quite the challenge. There is no room for error when executing manufacture of these patient specific therapeutics” — John Ibarra, Manufacturing Associate
Cleanrooms are highly valuable, particularly for ensuring clinical readiness and maintaining regulatory control. But the question facing the field now is: what comes next?
The Cost Equation
Cleanrooms don’t just limit scale – they add significant cost per batch.
Between infrastructure, environmental controls, gowning procedures, downtime between batches, and labor demands, cleanroom-based manufacturing drives up the cost of patient-specific therapies – often making them financially inaccessible for broader populations or health systems.
Key cost challenges include:
- High facility overhead per square foot
- Specialized labor and training requirements
- Inefficient scheduling, especially for one-batch-at-a-time models
- Process revalidation with every minor system or facility change
- Low throughput relative to demand in autologous programs
By contrast, closed, validated systems offer an opportunity to:
- Lower per-batch production costs
- Reduce downtime and cleanroom turnover
- Allow more predictable and distributed scheduling
- Open the window to more decentralization and manufacturing closer to delivery
- Support the reduction of logistical burdens of cell transport which could reduce viability and certainly adds cost
- Enable leaner staffing models with automation and digital oversight
“As part of the MSAT team, I focus on getting things ready before production — checking and writing material and equipment specs, reviewing cleaning and environmental Maintenance tickets for the pre and concurrent cleanroom processes, reviewing quality certificates, and making sure the paperwork is in place. For autologous batches, we still follow the same high standards you’d see for big production runs — same prep, same controls.
After production takes place, I periodically help review the post-run batch records. A lot is involved for each batch and I also know how expensive it is to run a cleanroom. With all the airflow, pass-throughs, and controls, it can cost $25,000 or more a month just in energy. That kind of facility setup makes sense when you’re making hundreds of doses when using the room, but probably not when you’re doing one batch for one patient. The cost can be lower by running multiple pod systems in one cleanroom, but in that case, the timing still depends on the room, not the patient. And that’s the real problem. We need to move toward closed systems that keep the same quality but give us more flexibility, so patients aren’t left waiting.” — Henry Sentmore, Scientist I, MSAT
While closed systems require upfront investment in platform development, validation, and integration, the long-term return in cost reduction, speed, and geographic reach is undeniable.
How Do We Get There?
Step One: Start Development with Closure in Mind
Many therapies begin at the bench in pre-clinical development, with flexible lab environments, outside the cleanroom entirely. These development spaces allow rapid iteration, protocol refinement, and side-by-side process comparisons.
“In early development, I focus on finding ways to simplify and tighten each step—because I know that eventually, someone will need to run this process repeatedly. Even small tweaks early on can make a big difference when you’re trying to close and scale later. Further, it is important to generate an overall process workflow to ensure there are no gaps from starting material storage, cleanroom process including multiple shifts when necessary and final product storage. In addition, to ensure reproducibility, a list of necessary documents such as a bill of materials including alternate approved suppliers, bill of equipment, a detailed process/batch record, and personnel training, (highly skilled, specialized training), must be a deliverable from transition of a project from development to manufacturing.” — Rogelio Zamilpa, PhD., Executive Director, Biomanufacturing & Collaborative Programs
That’s the challenge, and the opportunity. Even in early-stage work, teams should be evaluating how each unit operation can be transitioned into a fully closed, aseptically controlled format as the product matures.
Step Two: Transfer into Cleanrooms for Clinical Readiness
When therapies progress to clinical trials, the environment must evolve.
Cleanroom-based manufacturing becomes critical for:
- GMP compliance
- Controlled aseptic processing
- Documentation and QA required for regulatory submission
- Patient safety and product traceability
But this transition must be intentional. Teams must bridge what was developed flexibly into something that is now:
- Locked, validated, and reproducible
- Operated by trained staff in GMP workflows
- Documented with batch records and environmental monitoring
“Our job in MSAT is to get the process ready for this transition; functioning as a bridge between development and c GMP production, ensuring the process is efficient, robust, scaled appropriately while still maintaining quality across every batch. That transition from development to the c GMP environment is where a lot of risk lives, unless you have been planning for it from the beginning.” — Robert Reese, PhD.,Manager, Readiness, Manufacturing Science & Technology
Step Three: Engineer for Closure and Scale
Once a therapy is proven safe and effective, scaling the process for broader patient access becomes the priority. Cleanroom-based production, while effective, becomes a bottleneck for individualized therapies.
The next evolution requires:
- Fully closed, validated systems that operate without ISO 7 or ISO 5 room classifications
- Modular, replicable systems that can be deployed in new geographies
- Rapid Analytical Methods for real-time evaluation
- Digital process oversight, including remote monitoring and QA
- Supply chain models that minimize freeze-thaw and batch transit risks
“We’re seeing a convergence between medical device design and biomanufacturing. The future isn’t one massive facility; it’s interoperable systems that can be deployed near cell collection (leukapheresis) or delivery points. But to get there, we have to design processes now that will fit those future footprints. These may include deployment of stand-alone manufacturing mobiles that can deliver fresh and/or cryopreserved products including on-site validated analytical capabilities to minimize the time between manufacturing and product release. Further, streamlining the manufacturing process to efficiently and consistently deliver products shortest time possible is a must.” — Rogelio Zamilpa, PhD., Executive Director, Biomanufacturing & Collaborative Programs
Of course, transitioning from cleanrooms to closed systems isn’t a plug-and-play move. It comes with technical, regulatory, and strategic challenges that the field must navigate thoughtfully.
Dilemmas & How to Address Them
Here are a few common dilemmas, and how we believe the industry can respond:
Not all therapies are easily adaptable to fully closed systems:
- Some autologous processes may require partial openness. These can still benefit from hybrid cleanroom + closed system workflows that reduce risk and improve reproducibility.
Regulatory pathways for closed-system CGT manufacturing are still maturing:
- Early engagement with regulators and clear validation data, such as system challenge studies, environmental mapping, and aseptic assurance protocols—will be essential.
Development teams may over-optimize for the cleanroom environment:
- Shift the mindset early: “Build for transfer. Plan for closure.” Keep the end goal in mind even during preclinical development.
Devices and platforms vary in maturity and flexibility:
- This is where experienced partners can help, validating, integrating, and de-risking the system components to ensure comparability and scale-up readiness.
Qualifying and Validating The Closure
The move from cleanroom to closed-system requires:
- Validation of sterile connections and fluid paths
- Challenge studies that prove system integrity in worst-case conditions
- Regulatory alignment to show comparability and aseptic control
- Operator training and tech transfer support for new platforms
But it’s achievable and necessary if the field wants to expand access and affordability without compromising quality.
Mass Customization Without the Compromise
Other industries have already shown that highly personalized, high-quality products can be delivered at scale, not just through centralized factories, but through distributed, closed, and digitally coordinated systems.
For example, Align Technology produces over 320,000 custom dental aligners per day, each tailored to an individual’s digital scan. In eyewear, Zenni Optical makes more than 15,000 personalized prescription lenses daily, using automated milling and coating systems. Even 3D-printed orthopedic implants are now manufactured closer to the point of care, using distributed networks built on standardized, validated platforms.
These industries scaled by rethinking how, where, and by whom personalization gets delivered, without compromising safety or quality.
In cell and gene therapy, the path to scale looks different, but not impossible. Our field evolved under the expectations and infrastructure of traditional pharmaceutical manufacturing: central cleanrooms, tightly controlled suites, and large batch-based workflows. But that model wasn’t built for patient-specific care.
If we can decouple cleanroom infrastructure from the expectation of how advanced therapies must be produced, and instead embrace closed, automated, and modular systems, we open the door to scalable, decentralized, and truly accessible CGT manufacturing. Other industries have already made that leap. It’s time we imagine doing the same.
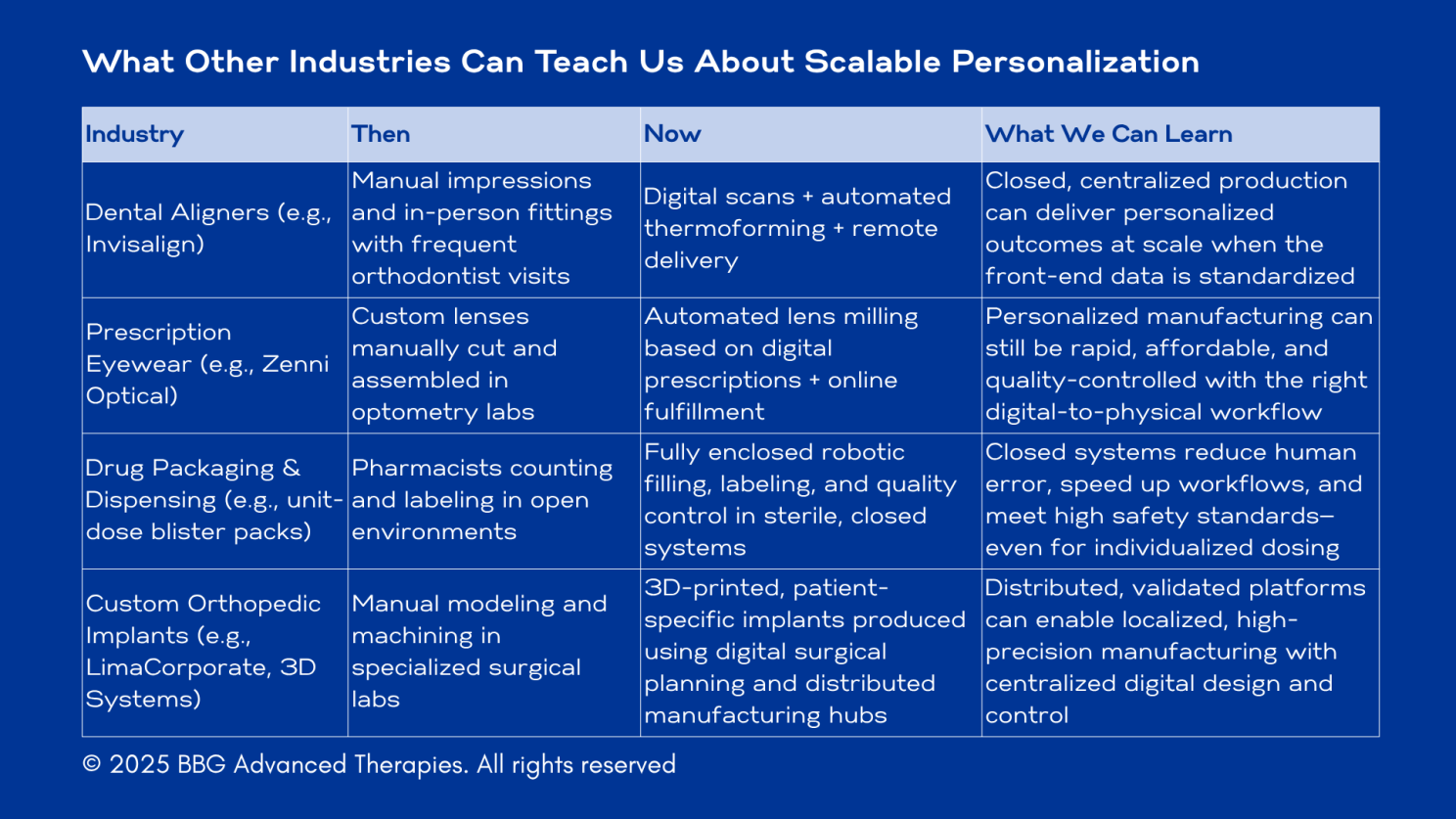
In all four examples, individualized service hasn’t gone away, but the complexity has shifted behind the scenes, into well-designed, automated systems that reduce cost and improve consistency.
Advanced therapy manufacturing is now approaching the same turning point:
- Inputs are patient-specific
- Precision is non-negotiable
- Access is not restrained – it’s broadly distributed
- But automation and closure can unlock scale
The takeaway? Custom doesn’t have to mean manual. Personalized doesn’t have to mean expensive. The right infrastructure can deliver both precision and reproducibility, at the scale patients need.
Final Thought
Patient-specific manufacturing may never be simple. But it doesn’t have to be inefficient.
Cleanrooms are a critical part of the journey, but they shouldn’t be the only destination. By designing for closure, planning for transfer, and building for scale, we can create a manufacturing ecosystem that matches the personalization of the therapies themselves.
It starts with asking one question early and often:
Can this process live outside the cleanroom, and still deliver GMP quality?
If the answer is yes, then that’s a future worth building.
Here to Help!
Our team at BBG Advanced Therapies collaborates with developers, platform innovators, and clinical programs to support process design and development, system qualification, validation, future planning, and infrastructure alignment.
Reach out to me, and the team at BBG Advanced Therapies if you’d like to talk through a challenge, test a concept, or build something scalable – together.
Visit bbgat.org, or contact us!

